This blog has a few aims and I’d like to set them down before anyone panics about what’s going to be said
- To try and encourage other midwives why it’s ok to bend the system – but only if it benefits the woman and her family
- To inspire others to be different and think outside the box 📦
- I’m telling my journey and not only what led me into midwifery but what keeps me there
- I want to show the media that midwives do care about women
- There will be no breaches of confidentiality
- The blog is of my thoughts and feelings
My life as a midwife began in 1982. I was a student nurse and on placement on a maternity unit learning about midwifery. I was sent into a room to watch a forceps birth – this was not in an operating theatre where complex forceps births take place nowadays but in a simple birth room – I can’t recall anything apart from the woman screaming and the way the forceps were used – it marked me for life so I don’t know how the woman progressed from it . I put off any thoughts of having my own children because of the way this woman seemed to suffer. Back then I was learning about life in the NHS , how to become a patients advocate , running my dad’s newsagents , continuing with my student nurse course which was run by the nursing school attached to the hospital . I was in shock afterwards and decided then I would never be a midwife .
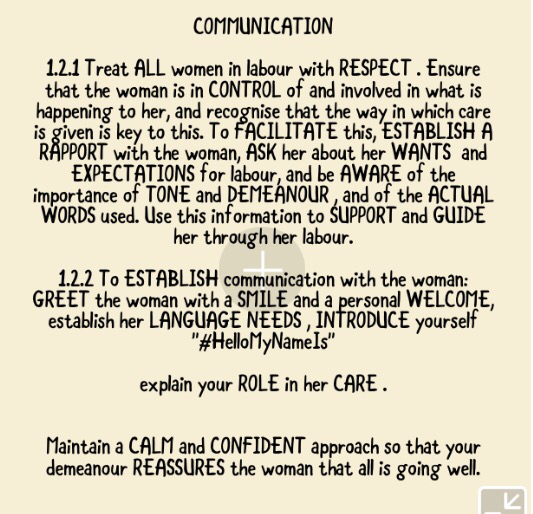
Fast forwards to the birth of my beautiful daughter in 1989 . I was admitted at 0.5cm dilatation and refused permission to go home because that’s how it was then – I was given a cervical sweep without being asked or consented for it and felt violated after the event asking the midwife “what did you just do to me ?” .
“I swept and stretched your cervix , you’ll labour now” was the reply – I didn’t know what to say and I was in pain but I accepted it and just felt lost .
I did eventually give birth 22 hours after my admission and struggled with the pushing part – the consultant was called in and I recall him shouting at me how to push and threatening me with forceps if I didn’t push harder . I gave birth on my back , semi – recumbent – no-one encouraged or suggested a change of position . I was GIVEN an episiotomy without consent and cannot recall any conversation about why this was DONE to me . More or less straight after my birth I was left alone with my daughter she was in skin to skin contact with me . This wasn’t because I knew about the benefits of skin to skin contact at all , but because I just didn’t want to let Jane go – my mums death when I was just 18 years old had impacted on me massively and I saw something in my daughter Jane’s face that reminded me of my darling mum , I was so emotional I couldn’t put Jane down – despite being encouraged to .
After the birth I developed bladder problems so had to be kept in for 5 days . I recall feelings of loneliness , sadness , especially when my partner and visitors left . There were strict visiting times in those days , no rule bending , no partners staying overnight allowed .
Once home I felt more relaxed but my partner was only given one day off work . I had no one, both my sisters were in high profile jobs and both my parents had died when I was younger . A friend came for a few hours a day and tucked me into bed with Jane , I slept whilst she tidied up , cooked and was there for me , I didn’t know what had hit me .
My community midwife Jean Duerden was amazing , I felt unwell had terrible perineal pain and couldn’t walk far – I accepted this as normal – I was a medical ward sister – I knew nothing about babies and / or petineums . My speciality was caring for men and women with medical conditions – a world apart .
My community midwife Jean realised something was wrong and I was quickly fast tracked and diagnosed with a perineal haematoma – my sutures were subcuticular and very difficult to release so I had to persevere with analgesia and antibiotics .
The visits from Jean my community midwife were the highlight of my days – she would bring a student midwife with her and we would talk about how I was feeling , the importance of rest and nutrition and emotional support . Jean also gave me brilliant Breastfeeding advice . One day I blurted out to Jean about my birth experience and she was amazing . I felt from my moments with Jean that she inspired me to become a midwife . Although my labour experience wasn’t great , my postnatal care was so different .
Almost three years later I started my midwifery training and I have to say despite the ups and downs , staff shortages , media portrayal of midwives , the difficulties I’ve gone through in my career I love being a midwife . My own experiences have shaped me and taught me to listen , act and trust women .
When I started my midwifery there were no computers – we wrote everything and risk management was very low key . I recall the Fire Officer teaching my group that the most important thing was to keep corridors clear and know which extinguisher to use in the event of a fire . This has stayed with me through my career and I get very upset when I see corridors with obstacles , I make it my mission to clear them .
I kept a diary and was so thankful to form a life long friendship on my course with another nurse called April . My tutor Anne Ivill suggested that we would get on and we are still good friends to this day . April went to work on neonatal unit as soon as she qualified and is now a health visitor working with children who have congenital illnesses and special needs . We don’t see each other as much as we should but when we do it’s like we’ve never been apart .
I’ve always been quirky and don’t like discipline or rules that restrict creativity, I was the same at school and used to get into trouble for standing up for friends who were unable to stand up for themselves . Once at high school a friend asked me to wait for her after a detention as she was scared of walking home on her own . We were barred from doing such things but I had a plan ! One of the teachers saw me on the corridor and asked what I was doing, I explained that I was waiting for Mr Heathcote to give me extra maths (a total lie). Mr Heathcote was found and my cover was blown – I had to stay late all week and clean all the desks in T6 (one of our classrooms) . I made those desks so clean and using my anger with myself as energy to get the job done – the relief was that I didn’t get extra maths I suppose ! 😂
So how has my life affected who I am as a midwife and a woman ? The most influential part of my life was growing up in a newsagents shop , talking to people from all walks of life and respecting them all as valued customers . I worked in the shop from a very young age because I mithered my parents to let me . At first I was only “allowed” to sell newspapers or one item sales . The best day was DECIMALISATION DAY . I had learnt a lot at school about this and was determined to help in the shop but my parents said no . I was so upset – then around 7.30 my dad called me into the shop they were struggling – I was to be allowed to help ! I recall elderly people asking me “how much is that in old money ?” And I dutifully exchanged prices bank to pounds , shillings and pence to help them understand . I can recall if I was off school that day or not but if I was in school I still went in as for my parents not to send me I would’ve had to be really unwell .
So I hope you enjoyed part one of my lifting the lid blog – in part two I will be referring to my student diary and how hard it was being the only one on the midwifery cohort with a young child.
To be continued ….,..
Thank you for reading
Love , as always
Jenny x ❤️