

Here it is my blog aimed at NHS managers and fundholders of maternity services – time to explain a few home truths. MORE support is required for midwives in the operating theatre from upper NHS management in order to facilitate and maintain SkinToSkin contact between mothers , fathers and babies .
A few reasons the midwife may have for leaving theatre include : –
- To check the placenta
- To take blood gases
- To obtain documentation from a printer (which is not actually in the operating theatre)
- To complete digital or written records
- To register the birth
Let’s look at it another way – if an operating department practitioner said to a midwife “I just need to nip out for a few minutes can you step in for me for a few minutes and help the anaesthetist? ” how would a midwife feel ? How often does this happen ? Never !!
We must respect each another’s professional competencies and abilities and not take advantage of any given situation . The operating theatre is governed by health and safety due to the highly clinical nature of its environment . Midwives are selling themselves short by trying to manage their workload instead of questioning why they need more support .
We must deal with the root cause which is midwives leaving theatre to complete routine tasks (when they should be staying with women and babies)
The symptom is the fear of other staff in theatre of caring for the dyad , the woman’s fear at being unable to speak out that she’s scared of holding her baby during her operation or procedure .
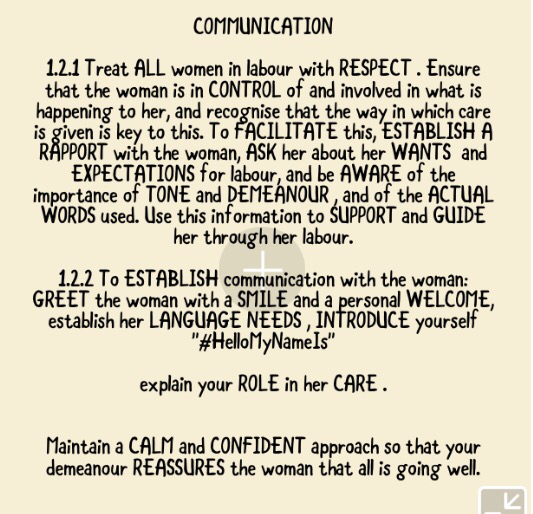
The midwife has a professional responsibility for the mother and her newborn as set out in the NMC code of conduct and The NMC Standards for Competence for Registered Midwives

I’d also like to refer to these key parts of the NMC code which seem to address care of the dyad in theatre so well .








If you are a manager support your midwives by auditing the reasons why a midwife might leave a woman in theatre for any length of time and address that issue with the multidisciplinary operating theatre team – there will be solutions and the solutions will improve care , safety , women’s and families experience of care in the operating theatre and well as giving midwives immense job satisfaction, plus enabling team cohesiveness – what more could you ask for ?
I am challenging all line managers to go into the operating theatre and watch the midwife – how can you make it better for the midwife and therefore the dyad ?
Keep on keeping on
Thank you for reading my blog
Please leave your comments as I appreciate all feedback
Jenny ❤️